

TL;DR:
- Bioactive dental materials actively exchange ions, stimulate biological responses, and promote remineralization at the tooth interface, unlike passive restoratives. A 2026 review shows they reduce secondary caries risk by about 45%, with glass ionomer cements providing the strongest evidence. Clinical use requires combining appropriate material selection with individualized risk assessment and supportive oral hygiene to optimize outcomes.
Most people assume that dental fillings and restorative materials simply occupy space in a damaged tooth. That assumption is outdated. Bioactive dental care refers to a category of materials and clinical strategies in which the dental material actively exchanges ions with the oral environment, stimulates biological responses, and promotes remineralization at the tooth interface. Understanding what is bioactive dental care, how these materials behave in vivo, and what the clinical evidence shows is increasingly relevant for patients weighing restorative treatment options that go beyond passive repair.
Table of Contents
- Key takeaways
- What is bioactive dental care: definition and core mechanisms
- Clinical benefits supported by the evidence
- Types of bioactive materials in dentistry
- How bioactive dental care works in clinical practice
- Common misconceptions about bioactive materials
- My perspective on where bioactive dentistry is headed
- Explore bioactive oral care options at Stop-oralcare
- FAQ
Key takeaways
| Point | Details |
|---|---|
| Bioactive materials are not passive | These materials release ions and form mineral layers that actively interact with tooth structure and surrounding tissue. |
| Secondary caries risk is measurably lower | A 2026 systematic review found a 45% reduction in secondary caries risk with bioactive restoratives compared to conventional materials. |
| Not all “bioactive” labels are equal | Biological effects depend on specific material class, ion release kinetics, and clinical context, not marketing terminology alone. |
| Bioactive care is a clinical strategy | Optimal outcomes depend on combining appropriate material selection with individualized risk assessment and supportive oral hygiene. |
| Glass ionomer cements lead the evidence | GICs currently show the strongest clinical data for caries prevention among bioactive restorative material classes. |
What is bioactive dental care: definition and core mechanisms
The term “bioactive” in dentistry carries a specific, scientifically grounded meaning. According to Larry Hench’s foundational bioactivity concept, true bioactivity requires a measurable biological response, such as the formation of an apatite mineral layer or the establishment of cellular bonding at the material-tissue interface. This is a more demanding standard than biocompatibility, which only requires that a material causes no harm.
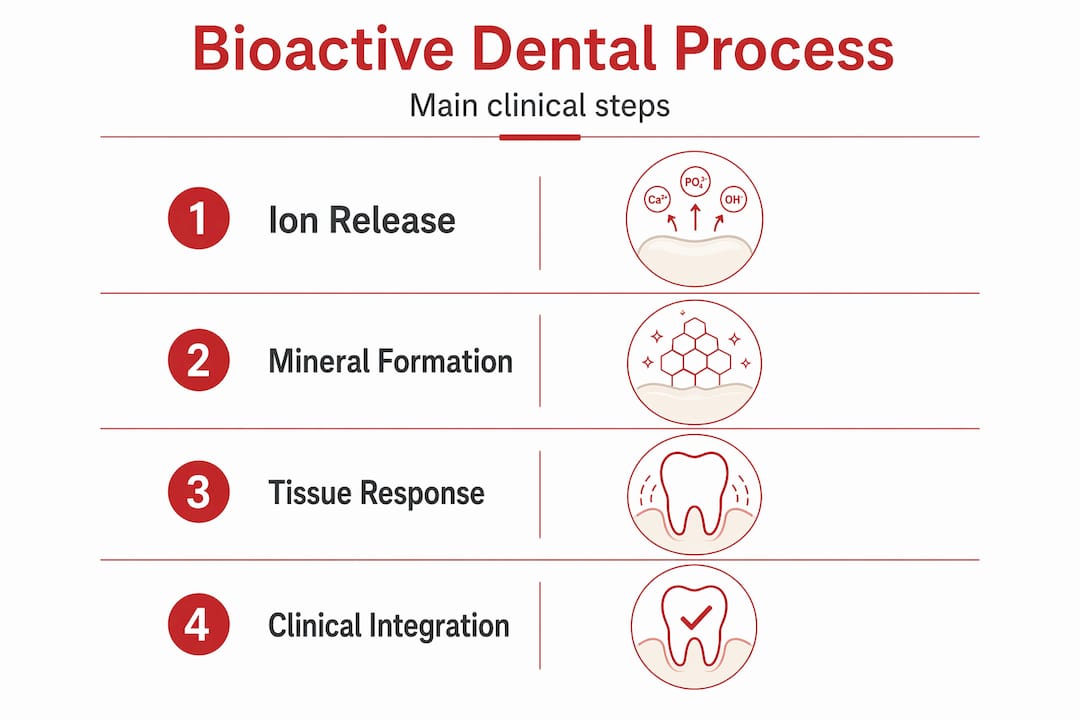
Bioactive dental materials achieve their effects through three primary mechanisms:
- Ion release. These materials release calcium, phosphate, and in some formulations fluoride ions into the surrounding oral fluid. These ions directly participate in mineral deposition on tooth surfaces and at the restoration margin.
- Apatite layer formation. When exposed to saliva or dentinal fluid, bioactive materials form a hydroxyapatite-like mineral layer. This apatite layer formation physically bonds the material to tooth structure and provides a continuous remineralizing reservoir.
- Biological response stimulation. Beyond mineral deposition, certain materials elicit cellular responses from pulpal cells and periodontal tissues, supporting tissue repair and bonding rather than simply filling a void.
It is worth distinguishing bioactive materials from materials that are merely ion-releasing or biocompatible. An ion-releasing material may not form a measurable apatite layer. A biocompatible material may be inert. Bioactive restorative materials sit in a distinct category defined by their capacity to elicit a specific, positive biological response. Understanding bioactive ingredients in oral care at this mechanistic level allows patients to evaluate clinical recommendations more precisely.
Pro Tip: Ask your dentist specifically which class of material is being used and what evidence supports its bioactivity. The phrase “bioactive” on a product label does not confirm that the material meets clinical bioactivity criteria.
Clinical benefits supported by the evidence
The clinical case for bioactive dental treatment has grown considerably. A 2026 systematic review analyzing 40 randomized controlled trials and over 5,500 restorations found that bioactive restorative materials reduce secondary caries risk by approximately 45% compared to conventional restorative materials. That is a clinically meaningful figure, particularly for patients with elevated caries risk.
The benefits of bioactive materials operate through several converging pathways:
- pH buffering. Ion release from these materials neutralizes acids produced by cariogenic bacteria, reducing the duration and severity of pH drops that drive demineralization.
- Remineralization support. Sustained calcium and phosphate release maintains supersaturation conditions at the tooth surface, favoring mineral deposition over dissolution.
- Bacterial deterrence. Bioactive resin composites reduce bacterial viability more than conventional resins, even when bacterial adhesion levels are comparable. This antimicrobial effect results from ion release rather than from added biocidal agents.
- Marginal integrity. The formation of a continuous hydroxyapatite layer at the restoration margin physically seals the interface, limiting microleakage that provides pathways for recurrent decay.
Glass ionomer cements currently hold the strongest evidence base among bioactive material classes. Newer bioactive dental products, including bioactive resin composites and giomers, show promise in emerging studies, though their long-term clinical data continue to develop. The practical implication is that material selection should be guided by the specific clinical scenario, the patient’s caries risk profile, and the available evidence for that particular material class rather than by category alone.
Patients interested in understanding the oral environment in which these materials operate can review the established science of dental biofilm dynamics, which directly informs why pH buffering and antimicrobial ion release matter in a restoration context.
Types of bioactive materials in dentistry
Bioactive materials in dentistry span several distinct classes, each with different compositions, mechanisms, and clinical applications. The following comparison presents the primary categories and their characteristics.

| Material class | Primary bioactive mechanism | Typical clinical applications | Relative mechanical strength |
|---|---|---|---|
| Glass ionomer cements (GICs) | Fluoride, calcium, phosphate ion release; apatite layer formation | Class III/V restorations, luting, pediatric fillings | Moderate |
| Resin-modified GICs | Ion release combined with resin polymerization | Posterior restorations, core build-up, liners | Moderate to high |
| Bioactive resin composites | Calcium phosphate or bioactive glass fillers releasing ions | Posterior and anterior restorations | High |
| Bioactive glass (silicate-based) | Ion release under acidic pH; mineral precipitation; antimicrobial action | Sealants, cavity liners, root canal sealers, implant surfaces | Variable |
| Calcium silicate cements | Calcium hydroxide and silicate ion release; pulp capping response | Vital pulp therapy, root-end filling, perforation repair | Low to moderate |
The ion-release profiles of these materials vary with oral pH and saliva chemistry. Under acidic conditions typical of active caries lesions, bioactive glass composites release ions at an elevated rate, providing a form of demand-responsive remineralization. Physical wear of the restoration surface also exposes fresh bioactive glass particles, which sustains the ion-release process over time.
Balancing mechanical strength and bioactivity represents a central challenge in material development. Silanization of fillers in resin composites improves durability but can reduce ion release. This trade-off means that material selection for high-stress posterior restorations requires careful consideration of both functional demands and therapeutic goals. Comprehensive prevention-centered dentistry resources offer additional context for understanding how material choice fits within broader restorative planning.
How bioactive dental care works in clinical practice
Understanding how bioactive dental care works requires placing material science within a clinical decision-making framework. The 2026 Frontiers clinical pathway paper situates bioactive and ion-releasing materials within minimum intervention dentistry and personalized caries management systems such as CAMBRA (Caries Management by Risk Assessment).
The clinical workflow typically proceeds as follows:
- Caries risk assessment. The clinician evaluates the patient’s biological risk factors, including salivary flow, diet, bacterial load, and history of caries, to classify individual risk level.
- Lesion activity evaluation. Active lesions present different treatment priorities than arrested lesions. Active cavitated lesions require operative intervention; active non-cavitated lesions may respond to noninvasive or microinvasive approaches.
- Material selection based on context. For operative restorations, the clinician selects a material class matched to the cavity location, occlusal load, and patient risk profile. High-risk patients with multiple active lesions benefit most from bioactive restoratives with sustained ion release.
- Adjunctive therapies. Bioactive restorative dentistry does not operate in isolation. Fluoride therapies, remineralizing rinses, dietary modification, and improved oral hygiene remain foundational. The combination of calcium, phosphate, and fluoride from multiple sources produces a synergistic remineralization effect.
- Monitoring and maintenance. Restoration performance and lesion activity are monitored at recall appointments to assess the clinical response and guide any necessary adjustments.
Pro Tip: Patients undergoing bioactive restorative treatment should maintain consistent fluoride and mineral supplementation at home. Bioactive materials perform best in an oral environment that supports remineralization rather than one dominated by persistent acidogenic bacteria.
Bioactive dental care functions best when it operates as a component of a personalized prevention strategy, particularly for patients with implants or complex restorative histories where secondary caries carries high clinical consequence.
Common misconceptions about bioactive materials
Several misconceptions complicate patient understanding of bioactive dental care. Addressing these directly supports more informed clinical discussions.
- “Bioactive” on a label guarantees specific biological effects. Not all labeled products deliver equivalent outcomes. Bioactivity is material-class specific. GICs, giomers, alkasites, and bioactive resin composites each have distinct efficacy profiles and clinical evidence bases.
- Bioactive materials eliminate the need for oral hygiene. Bioactive restoratives are therapeutic adjuncts. They do not replace plaque control, dietary management, or fluoride use. Materials perform best when lesion risk is actively managed through behavior.
- All bioactive materials work the same way. Ion release kinetics, the duration of sustained release, and the capacity for apatite layer formation differ substantially across material classes and even across products within the same class.
- Bioactive dental treatment is always the superior choice. For high-stress posterior restorations, mechanical performance requirements may favor materials with less bioactivity but greater fracture resistance. Clinical judgment, not a categorical preference, should guide selection.
The evidence base for bioactive materials continues to expand, and clinical guidance is evolving. Consultation with a dental professional who is familiar with the current literature on specific material classes remains the most reliable path to appropriate treatment selection.
My perspective on where bioactive dentistry is headed
I’ve watched the conversation around bioactive dental care shift noticeably over the past decade, and I’d argue the field is at a genuinely productive inflection point. The move from purely mechanical restoration toward biologically informed dentistry reflects a more accurate understanding of what teeth actually need from restorative materials. What I’ve seen in clinical practice confirms this: patients treated with glass ionomer-based approaches in high-risk contexts consistently show fewer secondary caries events than those restored with conventional composites under equivalent hygiene conditions.
That said, I’d caution against interpreting the 45% secondary caries reduction figure as a universal guarantee. That statistic reflects aggregate data across material classes and patient populations. Individual outcomes depend on lesion activity, salivary buffering capacity, and adherence to adjunctive care. The clinical evidence for bioactive materials is compelling but should be read with attention to which material classes generated the strongest results.
What I find most valuable about the bioactive paradigm is not any single material, but the shift toward thinking about restorations as therapeutic interventions rather than structural patches. That framing changes how clinicians approach risk assessment, material selection, and patient education. My experience suggests the real benefit comes from combining the right material with the right clinical strategy and realistic patient behavior goals, not from the material alone.
— Veronica
Explore bioactive oral care options at Stop-oralcare
Stop-oralcare has developed a line of natural oral care products formulated with mineral-rich compounds that support the same remineralization and ion-exchange principles underlying bioactive dental care. The product range, guided by Dr. Veronica Stahl’s expertise in dentistry and natural medicine, includes toothpastes, mouthwashes, and oral sprays designed to complement professional restorative treatment with at-home mineral support. For patients seeking scientifically grounded alternatives to conventional oral care, the full product catalog details ingredient profiles, clinical rationale, and usage guidance. Consulting a dental professional about integrating these products with your restorative treatment plan is strongly recommended.
FAQ
What does bioactive mean in dental care?
Bioactive dental materials actively release ions, form apatite mineral layers, and stimulate biological tissue responses rather than simply occupying the restoration space. This distinguishes them from inert or biocompatible materials that cause no harm but provide no active therapeutic benefit.
How effective are bioactive restorative materials?
A 2026 systematic review of 40 randomized controlled trials found that bioactive restoratives reduce secondary caries risk by approximately 45% compared to conventional materials, with glass ionomer cements showing the strongest evidence.
Are bioactive dental products safe?
Bioactive dental materials have undergone extensive clinical evaluation and are used routinely in restorative dentistry. Safety profiles vary by material class, and selection should be guided by a dental professional based on the patient’s specific clinical context.
Do bioactive materials replace fluoride treatments?
Bioactive materials complement fluoride therapy but do not replace it. Optimal remineralization outcomes result from combining sustained ion release from restorative materials with fluoride use and consistent oral hygiene practices.
How do I know if a product is truly bioactive?
Marketing terminology is inconsistent across the industry. Patients should ask their clinician which specific material class is being used and request evidence from peer-reviewed sources confirming the material’s ion release profile and clinical performance data.
Recommended
- Bioactive ingredients in oral care for sensitive teeth – Stop Oral Care
- Oral care ingredients guide: safe, natural solutions explained – Stop Oral Care
- Oral care science: principles, myths, and natural solutions – Stop Oral Care
- Biomimetic toothpaste: science-backed natural enamel protection – Stop Oral Care