

TL;DR:
- Oral bacteria can double every four to five hours, leading to significant microbial growth if brushing is missed. Evidence-based oral hygiene relies on scientifically validated tools and protocols to improve outcomes and reduce systemic health risks. Consistent, properly performed brushing and interdental cleaning grounded in research are essential for optimal oral and overall health.
Oral bacteria can double every four to five hours, which means a single missed brushing session allows microbial populations to expand significantly within the oral biofilm. Understanding what is evidence-based oral hygiene provides the scientific framework to interrupt this cycle with precision, rather than relying on habits inherited from tradition or marketing. This article examines the clinical research, validated tools, and practical protocols that define evidence-based dental care, offering readers a structured approach to oral hygiene practices grounded in peer-reviewed science and professional consensus.
Table of Contents
- Key Takeaways
- What is evidence-based oral hygiene
- Evidence-backed techniques and tools
- Misconceptions and unproven methods
- Daily application of evidence-based practices
- Oral hygiene and systemic health
- Expert perspective: what the evidence actually demands
- Natural oral care grounded in science
- FAQ
Key Takeaways
| Point | Details |
|---|---|
| Evidence-based definition | Oral hygiene grounded in peer-reviewed research, clinical guidelines, and patient-specific factors produces measurably better outcomes. |
| Brushing duration matters | Extending brushing from two to three minutes removes 55% more plaque, directly reducing disease risk. |
| Tool selection is validated | Powered oscillating-rotating brushes and interdental brushes show clinically superior plaque and inflammation control compared to manual alternatives. |
| Systemic connections are real | Periodontal disease is associated with systemic inflammatory conditions including diabetes and cardiovascular disease, making oral care a whole-body concern. |
| Professional care is non-negotiable | Home care alone cannot substitute for regular professional cleanings and examinations, which detect subclinical disease progression. |
What is evidence-based oral hygiene
Evidence-based oral hygiene is the disciplined application of the best available scientific research, integrated with clinical expertise and individual patient circumstances, to guide preventive and therapeutic oral care decisions. The concept originates from the broader framework of evidence-based medicine and was formally adopted in dentistry to move clinical practice away from tradition-based or anecdote-driven habits toward protocols validated by controlled clinical trials and systematic reviews.
The three foundational pillars of this approach are:
- Scientific evidence: Peer-reviewed studies, randomized controlled trials, and systematic reviews that assess the efficacy and safety of specific oral hygiene interventions.
- Clinical expertise: The professional judgment of dental practitioners who interpret and contextualize research findings within individual patient presentations.
- Patient values and preferences: Recognition that adherence depends on personal circumstances, dexterity, access, and comfort, making individualized guidance a component of evidence-based care rather than a deviation from it.
Integrating patient preferences with scientific evidence is explicitly recognized in clinical guidelines as a requirement for tailoring oral hygiene routines effectively. In daily practice, this translates to routine components that have been tested and validated: twice-daily brushing with fluoride toothpaste, daily interdental cleaning, appropriate mouth rinse use, and periodic professional examination.
Evidence-backed techniques and tools
Brushing frequency and duration
Clinical data consistently support brushing at least twice daily as the minimum threshold for effective plaque disruption. More precisely, 3-minute brushing removes 55% more plaque than a 2-minute session, which positions brushing duration as a modifiable and clinically meaningful variable. A soft-bristled brush applied with a systematic technique, covering all tooth surfaces and the gingival margin, produces the best outcomes.
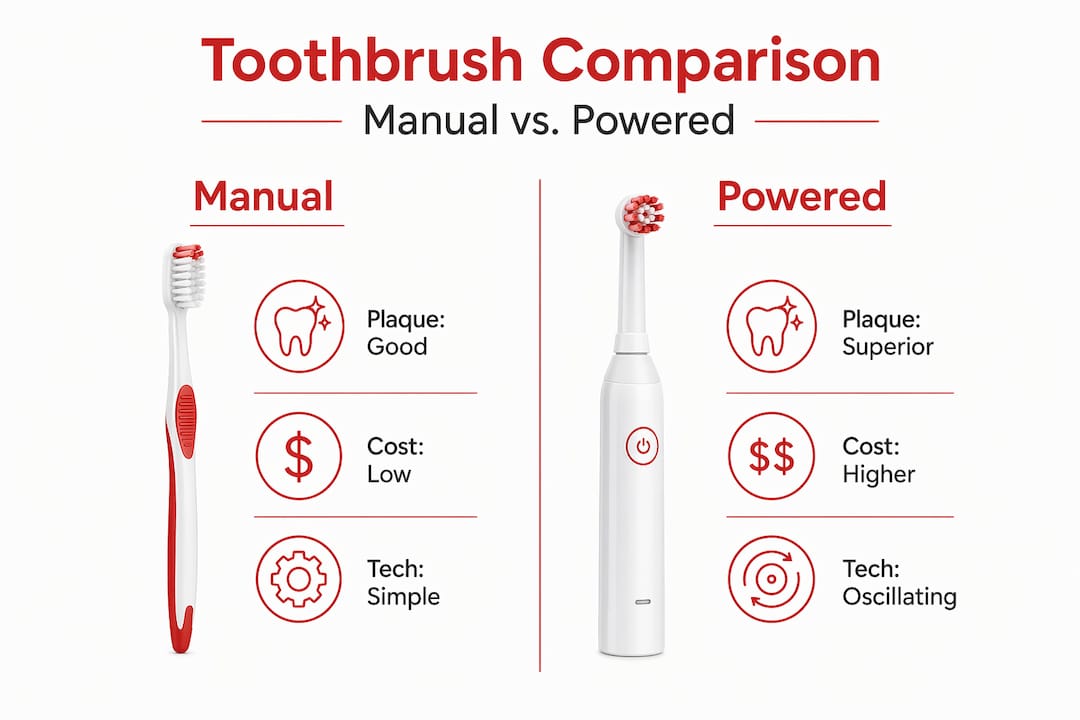
Powered versus manual toothbrushes
| Feature | Powered (oscillating-rotating) | Manual toothbrush |
|---|---|---|
| Plaque removal | Clinically superior | Effective with correct technique |
| Gingival inflammation | Reduced more consistently | Comparable with proper method |
| Caries prevention | No significant difference | No significant difference |
| Suitability | Recommended for limited dexterity | Appropriate for most users |
Electric and manual brushes show no significant difference in preventing dental caries across age groups, though oscillating-rotating powered devices improve plaque scores and reduce bleeding indices. The practical implication is that technique and consistency outweigh device selection for the majority of patients.
Interdental cleaning and adjuncts
Floss remains a widely recommended interdental cleaning tool, yet research indicates that interdental brushes and oral irrigators demonstrate superior plaque and inflammation control compared to traditional floss in clinical studies. For patients with wider interdental spaces, periodontitis, or dental implants, interdental brushes or water flossers represent a more effective choice.
Mouth rinses formulated with chlorhexidine or sodium fluoride carry documented antibacterial and anticaries effects. Clinical guidelines recommend these rinses specifically for high-risk groups, pregnant patients, and individuals undergoing periodontal therapy. Tongue scraping, while less discussed, can reduce odor-causing bacterial load by up to 75% according to clinical data, making it a defensible addition to a structured routine.
Pro Tip: Use a timer or a powered toothbrush with a built-in interval alert to accurately achieve three minutes of brushing. Most individuals significantly underestimate the time they spend brushing when relying on estimation alone.
Fluoride as primary caries-preventive agent
Fluoride strengthens enamel and reduces caries incidence across all age groups. Daily use of toothpaste containing at least 1,000 ppm fluoride is strongly recommended in current clinical guidelines. For individuals at elevated caries risk, professional fluoride varnish applications at 2.26% concentration provide additional protection beyond what home care alone can deliver.

Misconceptions and unproven methods
Not all popular oral hygiene practices have a basis in rigorous clinical evidence. Several widely adopted behaviors either lack validation or have been misunderstood in ways that compromise care quality.
- Emerging natural products: Many trending oral care products, including oil-pulling formulations, activated charcoal toothpaste, and various herbal rinses, lack the controlled trial data necessary for clinical endorsement. Experts consistently warn against adopting new interventions into routine care until they have been validated through high-quality research.
- Electric toothbrush superiority myth: Powered brushes offer incremental advantages in plaque reduction, but they do not compensate for poor technique or infrequent use. A patient who brushes manually for three minutes with a correct technique outperforms one who uses a powered brush for sixty seconds.
- Bleeding gums misattributed to brushing: Many individuals stop flossing when their gums bleed, incorrectly concluding that the tool is causing harm. Bleeding on initial flossing is a common inflammatory sign that typically resolves within seven to ten days of consistent interdental cleaning, as existing plaque accumulation decreases.
- Overconfidence in home care: No home regimen fully substitutes for professional examination and cleaning. Periodontal disease frequently progresses without symptoms, meaning clinical assessment is required to detect and manage subclinical pathology.
“Oral health education and simplified evidence-based protocols increase patient adherence and improve outcomes worldwide.” This finding underscores the value of clear, research-grounded guidance in motivating consistent oral hygiene behavior.
Daily application of evidence-based practices
Applying effective oral care methods consistently requires structuring a daily routine around validated intervals and tools. The following sequence reflects current clinical consensus.
- Morning brushing: Brush for two to three minutes with fluoride toothpaste following breakfast, covering all surfaces systematically. Spit but do not rinse immediately, allowing fluoride to remain in contact with enamel longer.
- Evening brushing and interdental cleaning: Conduct the most thorough session at night. Complete interdental cleaning before brushing so that dislodged plaque and debris are cleared by subsequent brushing.
- Mouth rinse use: Apply a fluoride or chlorhexidine rinse as directed based on individual caries or periodontal risk, typically after brushing and interdental cleaning at night.
- Tongue cleaning: Incorporate a tongue scraper as the final step to reduce bacterial load on the dorsal tongue surface.
- Professional examination schedule: Regular dental checkups every six months are recommended for most individuals, with higher-frequency visits indicated for those with active periodontal disease, elevated caries risk, or systemic comorbidities.
Pro Tip: When beginning a consistent flossing routine, mild bleeding is expected and should not prompt discontinuation. Persist daily for at least ten days. If bleeding persists beyond that window, consult a dental professional, as this may indicate active gingivitis requiring clinical intervention.
Lifestyle variables also modify the effectiveness of any oral hygiene protocol. Smoking increases periodontal disease risk by two to seven times, representing the largest single modifiable risk factor for gum disease. Dietary patterns, particularly high-frequency sugar intake, and systemic conditions such as diabetes further influence oral disease susceptibility. Incorporating a structured oral hygiene checklist into daily life supports consistency across all these variables.
For those exploring fluoride alternatives, a fluoride-free dental care protocol may offer supplementary options, though any substitution should be evaluated against current clinical evidence for caries prevention efficacy.
Oral hygiene and systemic health
The relationship between periodontal disease and systemic health is supported by a substantial and growing body of clinical literature. Several mechanisms have been proposed and partially validated through epidemiological and interventional research.
- Cardiovascular disease: Chronic periodontal inflammation contributes to systemic inflammatory burden, which is recognized as a risk factor for atherosclerosis and coronary artery disease.
- Diabetes: Bidirectional interactions exist between periodontal disease and glycemic control. Uncontrolled periodontal inflammation impairs insulin sensitivity, while poorly controlled diabetes accelerates alveolar bone loss.
- Adverse pregnancy outcomes: Periodontal disease during pregnancy has been associated with preterm birth and low birth weight in several prospective cohort studies.
- Nutritional compromise: Tooth loss and periodontal pain restrict dietary variety, disproportionately affecting intake of fibrous vegetables and proteins critical for systemic nutrition.
- Respiratory disease: Aspiration of oral bacteria, particularly in hospitalized or immunocompromised individuals, has been linked to pneumonia incidence.
Oral infections increase systemic inflammatory markers, with implications for chronic disease management across multiple organ systems. Viewing oral health as a component of holistic wellness, rather than an isolated specialty concern, is a position now reflected in major public health frameworks internationally. The oral microbiome, as a dynamic ecosystem, merits the same scientific attention given to the gut microbiome in contemporary medicine.
Expert perspective: what the evidence actually demands
In my clinical and research experience, the most significant barrier to evidence-based oral hygiene is not a lack of access to information. It is the persistent gap between what patients understand they should do and what they actually do consistently each day.
I have observed that many individuals correctly identify brushing twice daily as recommended, yet routinely brush for under sixty seconds and skip interdental cleaning for weeks at a time. The evidence does not merely suggest these steps. It quantifies their absence in disease outcomes. What I find most compelling about current research is not the novelty of the tools but the precision of the data on duration, frequency, and sequencing.
My clinical position is that simplified, evidence-grounded protocols are more effective than complex regimens. Patients who follow three well-understood behaviors consistently outperform those who attempt elaborate routines intermittently. The evidence on simplified protocols supports this directly. The future of evidence-based oral health practice lies in precision personalization: matching validated tools and agents to individual risk profiles rather than applying uniform population-level recommendations to every patient.
— Veronica
Natural oral care grounded in science
Stop-oralcare offers a curated line of natural oral health products formulated with hemp-derived compounds and Dead Sea minerals, developed under the scientific direction of Dr. Veronica Stahl. Each product is positioned within a framework of evidence-informed oral care, designed to complement validated hygiene protocols without replacing the foundational practices supported by clinical research. Readers seeking natural oral care options will find detailed product information, ingredient documentation, and guidance on integrating natural formulations into a structured oral hygiene routine. Stop-oralcare also maintains a body of educational content covering gum health approaches and safe oral care practices relevant to individuals seeking alternatives to conventional fluoride-based products.
FAQ
What is evidence-based oral hygiene?
Evidence-based oral hygiene is the practice of applying peer-reviewed clinical research, professional expertise, and patient-specific considerations to guide daily and preventive dental care decisions, replacing anecdotal or tradition-based habits with validated protocols.
How long should you brush your teeth according to research?
Current clinical data indicate that brushing for three minutes removes significantly more plaque than a two-minute session, with 55% greater plaque removal documented in comparative studies.
Are powered toothbrushes better than manual ones?
Oscillating-rotating powered brushes show marginal advantages in plaque reduction and gingival inflammation scores, but no significant caries prevention difference exists between powered and manual devices when technique is properly applied.
Why do gums bleed when flossing?
Bleeding during initial flossing typically reflects existing gingival inflammation caused by plaque accumulation, not tissue damage from the floss. Consistent daily flossing generally resolves this response within seven to ten days as inflammation subsides.
How does oral health affect overall body health?
Periodontal disease elevates systemic inflammatory markers and is associated with increased risk for cardiovascular disease, impaired glycemic control in diabetes, and adverse pregnancy outcomes, as documented in multiple prospective and interventional studies.
Recommended
- Natural teeth whitening: Evidence, safety, and dairy/hemp – Stop Oral Care
- Oral care ingredients guide: safe, natural solutions explained – Stop Oral Care
- What Is Botanical Oral Hygiene? Benefits and Expert Insights – Stop Oral Care
- Guide to Safe Oral Care 2025: Achieve a Healthier Smile – Stop Oral Care