

TL;DR:
- Many consumers misunderstand key oral care terms like enamel, plaque, and remineralization, affecting product choices.
- Nano-hydroxyapatite is an effective, fluoride-free mineral for enamel repair and sensitivity relief.
- Proper brushing techniques, such as the Modified Bass method, and understanding plaque versus tartar improve oral health outcomes.
Oral care language is frequently misapplied, even by individuals who maintain consistent hygiene routines. Terms such as enamel, plaque, remineralization, and gingivitis appear on product labels and clinical literature alike, yet their precise meanings are rarely understood by the consumers who encounter them daily. This disconnect between terminology and practical knowledge leads to suboptimal product selection and ineffective routines. The following guide provides clear, scientifically grounded definitions for the most critical oral care terms, with particular attention to how mineral-based and fluoride-free formulations interact with tooth structure at each stage of oral health.
Table of Contents
- Understanding your teeth: Enamel, dentin, and more
- What is plaque—and why does it matter?
- Gum disease decoded: From gingivitis to periodontitis
- Demineralization, remineralization, and the new science of natural repair
- Brushing, flossing, and modern routines: Making terminology actionable
- Why knowing the language of oral care leads to smarter choices
- Take the next step toward natural, modern oral care
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Enamel is mostly mineral | Ninety-seven percent of your enamel is hydroxyapatite, making mineral-based care essential. |
| Plaque vs. tartar | Plaque is soft and removable with good habits; tartar is hard and requires a dental professional. |
| Remineralization repairs damage | Adding minerals back to enamel helps repair early decay, with nHA as an evidence-backed option. |
| Technique matters more than tools | Proper brushing and flossing sequences, like the Modified Bass method, boost natural products’ effectiveness. |
| Knowing terms empowers choices | Understanding oral care language means you can pick safer, innovative products for your needs. |
Understanding your teeth: Enamel, dentin, and more
Let’s start by breaking down what makes up your teeth and why it matters for your daily routine.
The tooth is a layered structure, and each layer responds differently to oral care interventions. Understanding these layers is foundational to evaluating any product claim, particularly those involving mineral delivery or sensitivity relief. The four primary components of a tooth are enamel, dentin, pulp, and cementum, each with a distinct composition and functional role.
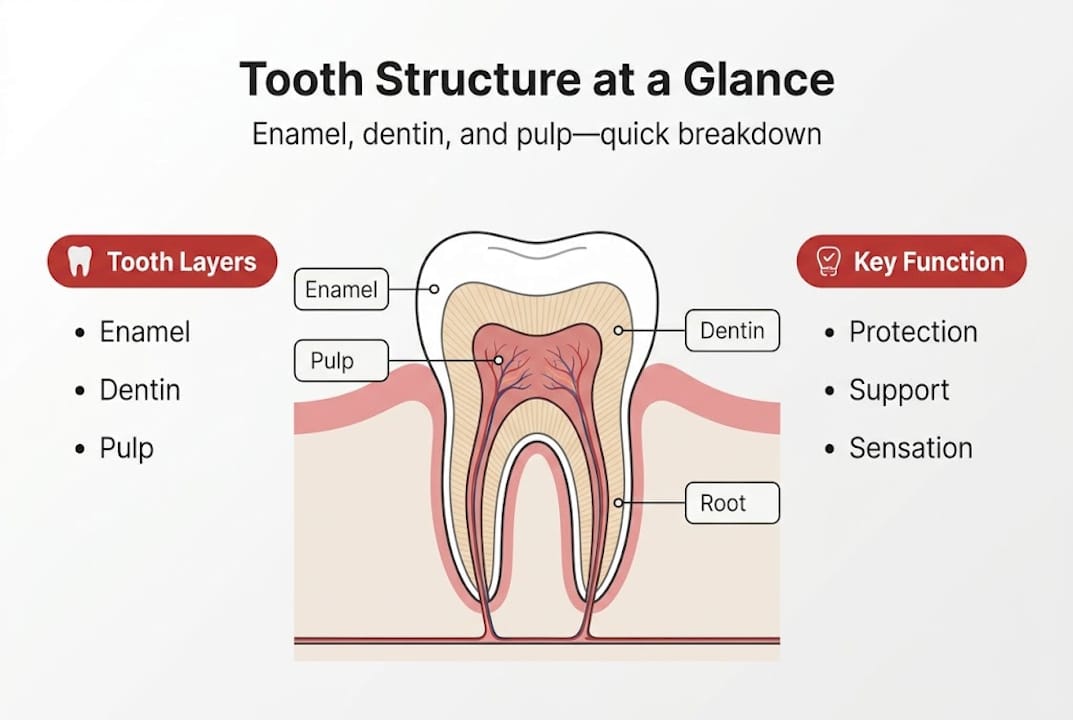
Enamel is the outermost, visible layer of the crown. It is the hardest biological tissue in the human body, and enamel comprises 97% hydroxyapatite mineral, making it highly susceptible to acid-driven mineral loss. Because enamel lacks living cells, it cannot regenerate on its own once significantly damaged. This is why the mineral composition of oral care products matters so much.
Dentin lies beneath the enamel and constitutes the bulk of the tooth. It contains approximately 70% hydroxyapatite and 20% organic material, primarily collagen. Dentin is traversed by microscopic tubules that connect to the pulp, which explains why exposed dentin causes sensitivity to temperature and pressure.
Pulp is the innermost soft tissue containing nerves and blood vessels. It is responsible for tooth vitality and sensation. Cementum covers the root surface, anchoring the tooth to the periodontal ligament and underlying bone.
Key structural facts worth noting:
- Enamel thickness varies from 2.5 mm at the cusp to near zero at the gumline
- Dentin tubules number approximately 15,000 to 65,000 per square millimeter
- Cementum is softer than both enamel and dentin, making root surfaces particularly vulnerable
- Pulp volume decreases with age as secondary dentin forms
| Tooth layer | Primary composition | Key function |
|---|---|---|
| Enamel | 97% hydroxyapatite | Protective outer surface |
| Dentin | 70% hydroxyapatite, 20% collagen | Structural bulk, sensation |
| Pulp | Nerves, blood vessels | Vitality and sensation |
| Cementum | 45% hydroxyapatite | Root anchorage |
Nano-hydroxyapatite (nHA) is a biomimetic mineral engineered to match enamel’s natural composition. It integrates directly into enamel defects, supporting remineralization without the systemic concerns associated with fluoride. Consumers interested in hydroxyapatite for sensitive teeth will find that nHA’s mechanism of action is rooted in this structural compatibility with the tooth’s own mineral matrix.
What is plaque—and why does it matter?
Now that you know the basics of your teeth, let’s tackle one of oral care’s most misunderstood but most important topics: plaque.
Plaque is a sticky bacterial film; calculus is hardened plaque requiring professional removal. These two terms are often conflated, but the distinction is clinically significant. Plaque is a dynamic, living biofilm that forms continuously on tooth surfaces. Calculus, also called tartar, is mineralized plaque that has hardened and adheres firmly to enamel and root surfaces.
Plaque forms through a predictable sequence. Within minutes of brushing, salivary proteins coat the tooth surface, forming the acquired pellicle. Early colonizers such as Streptococcus mutans attach to this pellicle and begin producing acids as metabolic byproducts of carbohydrate fermentation. Within 24 to 48 hours, a structured biofilm develops. If not disrupted by mechanical cleaning, this biofilm matures and mineralizes into calculus within approximately 10 to 14 days.
The health consequences of unmanaged plaque include:
- Enamel demineralization from sustained acid exposure
- Gingivitis from bacterial toxins irritating gingival tissue
- Periodontal disease progression if calculus accumulates subgingivally
- Halitosis from volatile sulfur compounds produced by anaerobic bacteria
“Plaque is a polymicrobial biofilm, not simply a surface deposit. Its structural complexity makes mechanical disruption the primary and most evidence-supported method of control.”
Strategies for natural plaque management focus on consistent mechanical disruption rather than chemical suppression alone. Effective approaches include twice-daily brushing with a mineral-rich formulation, interdental cleaning, and the use of botanically active rinses. Guidance on removing plaque naturally outlines step-by-step protocols that combine mechanical and mineral-based methods. For individuals seeking adjunctive support, evidence also supports the role of mouthwash for plaque removal as part of a structured routine.
Gum disease decoded: From gingivitis to periodontitis
With plaque and tartar addressed, let’s move on to what happens if these aren’t managed: gum disease.

Gingivitis presents with red, swollen, bleeding gums; periodontitis causes bone loss and is classified as advanced disease. These two conditions represent a continuum, not separate diseases. Gingivitis is fully reversible with proper oral hygiene. Periodontitis, however, involves irreversible destruction of the alveolar bone and periodontal ligament.
The progression from gingivitis to periodontitis follows a recognized sequence:
- Plaque accumulation at the gingival margin triggers an inflammatory response
- Gingival tissue becomes edematous, erythematous, and bleeds on probing
- If unaddressed, bacterial toxins penetrate the sulcus, forming a periodontal pocket
- Pocket depth exceeding 3 mm indicates disease progression beyond gingivitis
- Alveolar bone resorption occurs as the immune response damages supporting tissue
- Advanced periodontitis results in tooth mobility and potential tooth loss
Recognizing the terminology distinction between gingivitis and periodontitis matters when evaluating product claims. A product marketed for “gum health” may address early-stage inflammation but will not reverse established periodontitis. Consumers benefit from understanding that early intervention, guided by accurate terminology, yields the best outcomes.
Pro Tip: Bleeding gums during brushing are not normal and should not be dismissed. They are a clinical indicator of gingivitis and a signal to reassess your routine before disease progresses.
Mineral-based and botanical formulations show particular promise at the gingivitis stage. Dead Sea minerals, for instance, contain magnesium, potassium, and calcium in concentrations that support tissue health and reduce inflammatory markers in early gum disease. Detailed protocols for natural gum disease prevention provide evidence-referenced approaches for managing early-stage disease without conventional chemical agents.
Demineralization, remineralization, and the new science of natural repair
To truly understand how to keep your teeth healthy, you need to know how minerals move in and out of your enamel.
Remineralization deposits minerals into demineralized enamel; demineralization occurs below pH 5.5. These two processes operate in dynamic equilibrium throughout the day. Every acid challenge from food, beverages, or bacterial metabolism tips the balance toward demineralization. Saliva, along with mineral-rich oral care products, works to restore that balance.
Demineralization begins when oral pH drops below the critical threshold of 5.5. At this point, hydroxyapatite crystals in enamel begin to dissolve, releasing calcium and phosphate ions. Early demineralization appears as white spot lesions, which are the first visible sign of caries development. At this stage, the process is still reversible.
Nano-hydroxyapatite directly fills enamel defects and shows equivalent or superior remineralization to fluoride in microhardness recovery studies. This positions nHA as a scientifically credible fluoride alternative, particularly for populations seeking fluoride-free formulations.
| Property | Nano-hydroxyapatite (nHA) | Fluoride |
|---|---|---|
| Mechanism | Biomimetic mineral integration | Converts hydroxyapatite to fluorapatite |
| Remineralization | Direct mineral deposition | Enhances mineral uptake indirectly |
| Sensitivity relief | Occludes dentinal tubules | Limited direct effect |
| Safety profile | Biocompatible, non-toxic | Systemic concerns at high doses |
| Fluoride-free | Yes | No |
Pro Tip: Look for nHA listed as “nano-hydroxyapatite” or “n-HAp” on ingredient labels. Concentrations between 10% and 15% are associated with the strongest clinical evidence for remineralization.
For a detailed scientific comparison, the analysis of nHA vs fluoride toothpaste examines peer-reviewed data across multiple clinical outcomes.
Brushing, flossing, and modern routines: Making terminology actionable
Having learned the science, let’s make sense of everyday routines and the jargon that comes with them.
The Modified Bass technique uses a 45-degree angle to the gumline with small vibratory motions for two minutes and is considered the most effective method for gingival plaque removal. This technique targets the gingival sulcus directly, which is where plaque accumulation poses the greatest risk for gingivitis and early periodontal disease.
To apply the Modified Bass technique correctly:
- Position the brush at a 45-degree angle to the gumline, with bristles contacting both tooth surface and gingival margin
- Apply light pressure and use short, vibratory strokes covering two to three teeth at a time
- Move systematically around all four quadrants, spending approximately 30 seconds per quadrant
- Brush all surfaces: buccal, lingual, and occlusal
- Maintain consistent light pressure to avoid gingival abrasion
Interdental cleaning is equally important. Flossing before brushing dislodges debris for better efficacy; spit don’t rinse after nHA to allow remineralization. Flossing first ensures that loosened interproximal debris is subsequently removed by brushing, rather than redistributed. The “spit don’t rinse” protocol preserves the active mineral concentration on tooth surfaces, allowing remineralization to continue after brushing.
Pro Tip: Interdental brushes are more effective than floss for individuals with wider interproximal spaces or periodontal pockets. Select a size that fits without forcing, and use them before your primary brushing step.
For those incorporating mineral-based products, step-by-step guidance on using a natural plaque remover provides protocol-level detail for integrating these tools into a structured, evidence-supported routine.
Why knowing the language of oral care leads to smarter choices
Stepping back, here’s why decoding these terms truly matters on your journey to better oral health.
The oral care market is saturated with terms that function as marketing signals rather than scientific descriptors. Words like “whitening,” “advanced protection,” and “natural” carry no standardized clinical definitions. Consumers who lack precise terminology are effectively unable to evaluate these claims on their merits.
Understanding the distinction between remineralization and whitening, or between gingivitis and periodontitis, allows for genuinely informed product selection. It also reveals why certain formulations are better suited to specific clinical needs. A product containing nHA addresses demineralization at the enamel surface. A product marketed solely for whitening may not.
The evidence base for fluoride-free mineral solutions has grown substantially. Consumers who understand what nHA does mechanistically are better positioned to assess whether a product’s ingredient list supports its claims. The comparative analysis of fluoride vs nHA evidence illustrates precisely this point: terminology literacy translates directly into the ability to distinguish evidence-based innovation from marketing language.
Take the next step toward natural, modern oral care
Ready to put your new knowledge to work? Here’s where to start.
The terminology covered in this guide reflects the scientific foundation behind a new generation of oral care products. Formulations incorporating nHA, Dead Sea minerals, and hemp-derived botanicals are not simply alternatives to conventional products. They are products developed in response to specific gaps in the clinical evidence for traditional ingredients.
Stop Oral Care offers a line of natural, fluoride-free oral care products formulated with precisely these evidence-based ingredients. Each product is developed with reference to current research on remineralization, biofilm management, and gingival health. Whether you are addressing early enamel loss, managing gingivitis, or seeking a fluoride-free daily routine, the product range is designed to align with the science you now understand.
Frequently asked questions
What is the difference between plaque and tartar?
Plaque is a soft bacterial film; tartar is hardened plaque that adheres to tooth surfaces and requires professional removal to eliminate. Daily brushing and flossing disrupt plaque before it can mineralize into tartar.
How does remineralization repair teeth?
Remineralization deposits minerals into enamel, reversing early demineralization and restoring microhardness before cavities can form. Mineral-rich toothpastes and a balanced oral pH support this process daily.
Is nano-hydroxyapatite safe and effective?
nHA is biocompatible and remineralizes enamel with effectiveness comparable or superior to fluoride in clinical studies, while also reducing dentinal sensitivity. It is considered safe for all age groups, including children.
What is the Modified Bass brushing technique?
The Modified Bass technique positions bristles at 45 degrees to the gumline and uses gentle vibratory strokes for two minutes to maximize plaque removal at the gingival margin. It is the most evidence-supported brushing method for gum health.
Should I spit or rinse after brushing with fluoride or nHA toothpaste?
You should spit but not rinse after brushing to preserve the active mineral concentration on tooth surfaces and allow remineralization to continue. Rinsing immediately after brushing significantly reduces the protective effect of both fluoride and nHA formulations.
Recommended
- Oral care ingredients guide: safe, natural solutions explained – Stop Oral Care
- Top natural oral ingredients for healthier teeth and gums – Stop Oral Care
- Oral care science: principles, myths, and natural solutions – Stop Oral Care
- Natural Ingredients In Dental Care – Why They Matter – Stop Oral Care